

Weight loss means that an animal has been losing weight or body condition score over a period. Weight loss is more noticeable when acute, but it may be more difficult to identify initially if the loss of body condition score or weight is progressive and sustained in time.
In general, for domestic populations of leisure horses with daily access to pastures, a body condition score (BCS) of 5/9 on the simplified 9-point system for body condition scoring horses (Kohnke, 1992; Renelle et al, 2018) is considered ideal. The use of the horse should be considered to determine the ideal BCS (Mair, 2002). Seasons have an important effect on BCS and weight. For a leisure horse with daily access to pastures in the UK, a BCS of approximately 6/9 is expected in summer and around 4/9 in late winter (Giles et al, 2014). It should be considered that, depending on the husbandry and working conditions, seasonal variations may differ. For instance, in a study on thoroughbred horses kept on a diet with a constant energy intake throughout the year, the BCS of males peaked in autumn and winter and reached a nadir in spring, whereas the BCS of mares peaked in autumn (Takahashi and Takahashi, 2017). Furthermore, breed, use, sex, physiological status (for example, pregnancy or lactation status) and extreme weather events have an impact in the seasonal variation of BCS and weight (Brinkmann et al, 2012).
Taking this information into account, it is reasonable to first ask the question of whether changes in body weight and condition score may be related to physiological needs. Ideally, one should try to objectively quantify losses in body weight and BCS. In order to do so, horses should be weighed regularly using an appropriate scale or measuring tape. It should be considered that depending on the horse and the measuring tape, weight can be under or overestimated. Hence, it is important to use the same tape to perform serial measurements in any given horse. The tape will be useful in estimating body weight changes, rather than providing an accurate estimate of current body weight. BCS should also be evaluated regularly following the simplified body condition scoring system by Kohnke (1992).
Weight loss is determined by a balance between intake, absorption, utilisation and loss of nutrients. Any alteration in the balance of these components will affect the ability of a horse to maintain its normal weight. The main pathophysiological mechanisms of weight loss include decreased dietary intake, increased rate of utilisation or loss of nutrients, malabsorption or maldigestion, inadequate delivery to tissues and conditions that cause muscle wasting (Tamzali, 2006, Hund, 2020). It is possible for horses to experience loss of weight as a result of a combination of two or more of the aforementioned mechanisms, or to have two or more concurrent aetiological factors causing weight loss in one individual animal. This is most seen in geriatric patients where comorbidities are more common (Ireland et al, 2014; Jarvis and McKenzie, 2021). For example, protein calorie malnutrition owing to poor dentition may be compounded with increased energy requirement in an animal with chronic respiratory problems, or with protein losses caused by chronic renal disease (Jarvis, 2021). Weight loss can occur as a result of inadequate nutrient intake, but can also occur despite animals presenting with normal appetite and eating adequate amounts of quality feed (Metcalfe et al, 2013). Common causes of weight loss in horses include protein calorie malnutrition, dental problems and endoparasites. However, once these are ruled out, the spectrum of problems causing weight loss can be broad and, in some cases, may indicate the presence of severe illness (Metcalfe et al, 2013).
Given the clinical relevance of weight loss, the equine clinician is faced with important questions that need to be answered. A systematic approach to weight loss should be followed in all cases. Figure 1 summarises the suggested workflow for horses with weight loss.
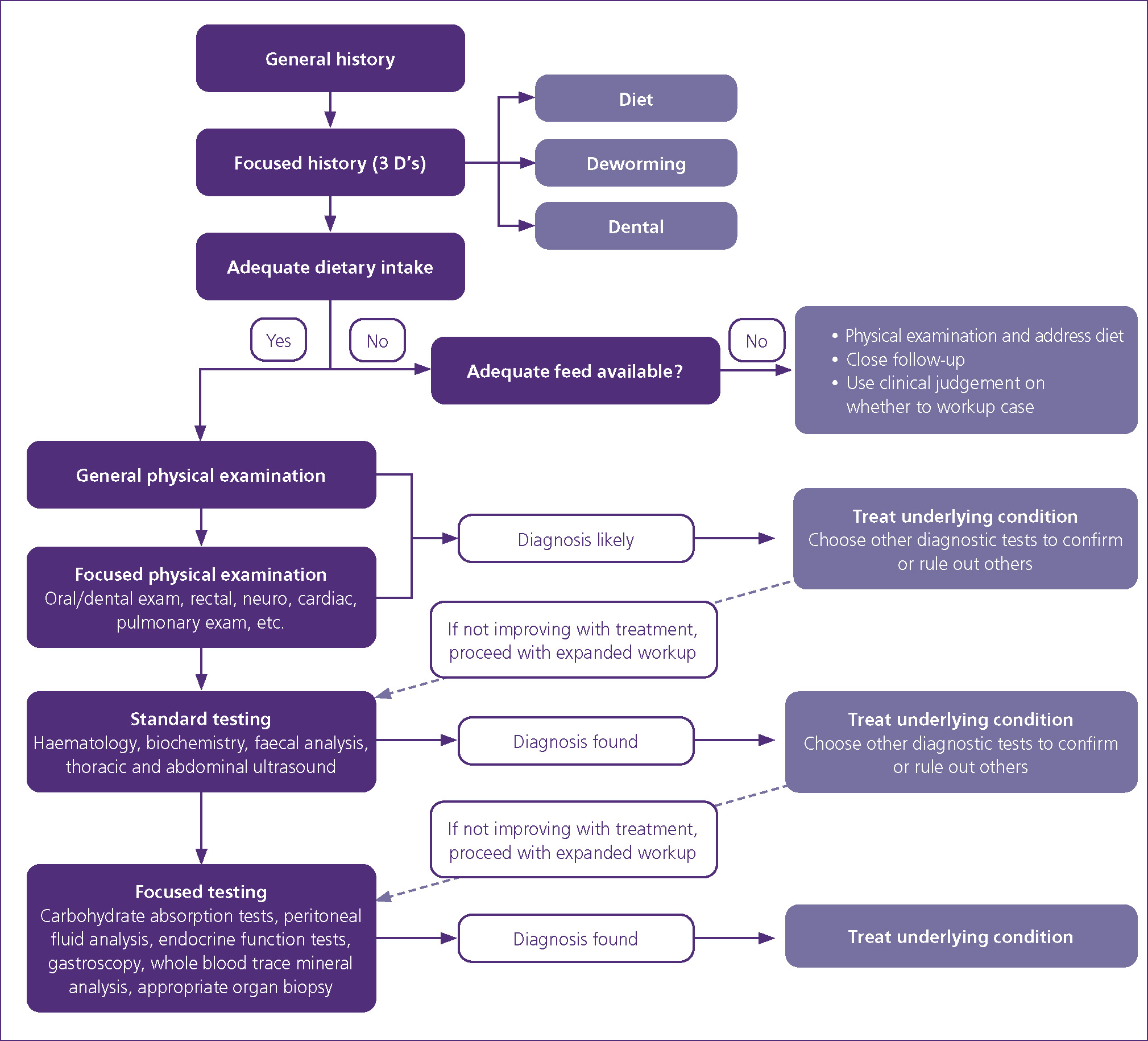
General and focused history
A general history will provide vital information to help determine if weight loss is related to undernutrition or not. Obtaining detailed information should help determine whether the horse has an adequate dietary intake (ask about social interactions and pecking order), if it is being offered a correct amount and quality of feed, and if the animal has a normal appetite, or presents with partial or complete anorexia. An emphasis should be put on gathering information about diet (review daily amount as well as meal sizes), deworming, dental problems and routine dental care. A history focused on these three aspects aims to identify a set of issues that account for a high proportion of cases of weight loss in the horse. One should evaluate the owner’s perception about the BCS of the patient and take into consideration their perspective in order to assess the changes in BCS over time.
Diet
Undernutrition is probably one of the most common causes of weight loss in the general equine population. In cases of weight loss, it is important to estimate individual nutrient requirements and real intake. It is also important to perform a complete nutritional assessment of the horse. Diet and the management of diet need to be assessed; Table 1 outlines some of the important aspects to take into consideration when evaluating diet history. It must be acknowledged that there are individual variations in the ability to maintain weight and BCS among horses, for example horses with differing metabolic tendencies that are colloquially referred to as ‘easy keepers’ and ‘hard keepers’. Evidence shows that there are significant faecal microbiome differences between these groups of horses, as well as horses that are classified as ‘medium keepers’ (Johnson and Biddle, 2021).
Table 1. Important aspects to take into consideration when evaluating diet history in adult horses with weight loss
| Diet/ration | Feeding management |
|---|---|
|
|
*Steamy and many seeds is mature, soft without seed is immature
†Steamy forage inadequate for underweight horses
For hard keepers, digestible energy and other nutrient requirements are higher. These differences should be considered when evaluating and formulating appropriate diets. A standard scale to measure the keeper status of individual horses has been developed (Johnson, 2021). The diet for ‘hard keepers’ should be evaluated carefully and reformulated if necessary.
Deworming
Deworming history might provide important information pertaining to weight loss, as in certain situations, very high parasite burdens can be a contributing factor. Very high, large strongyle burdens are rarely encountered in well managed equids, and most clinically relevant cases are related to neglected horses or horses with poor management. Anaplocephala spp. do not compete for nutrients and rarely cause enough damage to the large intestinal mucosa to contribute to loss of weight. However, there is ample evidence linking anaplocephala infestation to colic, mainly as a result of lesions to the mucosa, submucosa, hypertrophy of the circular muscle layer at the ileocecal junction and injury to the enteric nervous system around the ileocaecal junction with moderate to high parasite infestation (Pavone et al, 2010; Back et al, 2013). This is true as sporadically, horses may develop ileocecal intussusception or caecum base pathology in the presence of a relatively small amounts of Anaplocephala spp. parasites. However, the number of parasites required to effectively alter motility or to cause enough damage to the intestinal wall as to cause clinical complications is unknown. A reliable ELISA test for the detection of tapeworm infestation using either saliva or serum in horses is available. The test has demonstrated moderate to high sensitivity and specificity in horses with moderate and heavy parasite burdens respectively (Lightbody et al, 2016).
Small strongyles on the other hand tend to be more problematic, even in well managed populations. There is evidence of emergence of drug-resistant cyathostomines to widely used antihelmintics in the UK, as evidenced by a shorter egg reappearance period (Molena et al, 2018). Cyathostomins can be of particular importance when arrested fourth stage larvae emerge in large numbers causing diarrhoea and systemic inflammation, secondary to large colon and caecum inflammation (Love et al, 1999; Steinbach, 2006). Small strongyles would theoretically have a more pronounced effect on weight and body condition score in horses whose diet is mainly composed of roughage, compared to feed supplementation that is digested in the small intestine (Silva et al, 2016). In an experimental study, the deworming agent fenbendazole used against small strongyles caused inflammation in the large intestinal mucosal, favouring the use of moxidectin (Steinbach et al, 2006). In another study, differences in mucosal inflammation reaction after treatment with fenbendazole or moxidectin were very subtle (Steuer et al, 2018). However, moxidectin, apart from being highly effective against all stages of small strongyles, also provides a persistent activity against re-infection (Corning, 2009). A faecal egg count should be repeated once a day for five consecutive days in cases of suspected cyathostomine infestation, to improve the sensitivity of the test. A positive faecal flotation or sedimentation test, a positive ELISA test (for tapeworms), or the presence of parasites in faeces are clear indications for the administration of anthelmintic drugs. In some patients, a test of treatment with larvicidal anthelmintic drugs is used after other causes of weight loss have been ruled out. Tamzali (2006) recommends performing daily faecal analysis during the 5 days after treatment is started in order to confirm the diagnosis of cyathostomin infestation.
Dentition
Dental problems are a potential cause of oral dysphagia and anorexia. Modern texts cite dental problems as a cause of weight loss (Reed et al, 2016). It is obvious that there is a great benefit in treating pathological conditions of the teeth and soft tissues of the oral cavity through interventional dentistry in horses (Carmalt et al, 2007). However, few studies have investigated the effects of routine occlusal dental equilibration and weight gain in horses (Carmalt et al, 2004, 2007). Nonetheless, dental problems should always be considered in cases of weight loss, particularly in geriatric patients. Careful dental examination should be performed in horses with weight loss.
Undernutrition
If it is determined that the problem is related to undernutrition, a nutritional plan addressing the dietary problems should be undertaken. To evaluate and adjust the diet, a clinical nutritionist should be contacted for ration formulation. The use of commercial equine nutrition calculators (such as www.FeedXL.com) can be helpful. However, the use of a commercial calculators is not a substitute for knowledge and expertise in equine nutrition. A general physical examination should be performed, and clinical judgement should be used to determine if further diagnostic work-up is necessary on an individual basis.
Table 2. Suggested standard and specialised tests for the diagnostic work-up of adult horses with weight loss
| Standard testing | Specialised testing |
|---|---|
|
|
General and focused physical examination
An exhaustive physical examination should be performed in all horses with weight loss. Objective weight measurement and an estimation of the BCS should be recorded. The general physical examination should provide an idea of major clinical signs and guide the clinician toward a thorough, focused physical examination of specific body systems. Abnormal coat, musculoskeletal or dental problems, diarrhoea, cardiac and respiratory abnormalities, or oedema, should be noted.
In addition, horses should be watched while eating the different types of feed they consume regularly. Horses should also be watched eating using their regular feeding systems, at the same location, with their herd companions. Horses may show difficulties prehending concentrate. However, prehension problems may be missed with roughage. Care should be taken to determine if water or food comes out of the nostrils. In cases of mild, partial dysphagia, this might not be particularly evident unless careful observation is performed. A rectal examination often provides valuable information and should always be included as part of the work-up of horses with weight loss (Tamzali, 2006).
After performing a rectal examination, a sedimentation test of the faeces should be performed looking for sand or gravel. A small amount of sand in the faeces is normal. However, large quantities are suggestive of sand impaction. If after general and focused physical examination a potential cause of weight loss is identified, the clinician should start treating the underlying condition. If deemed necessary, additional tests to confirm or rule-out other conditions should be undertaken.
Standard testing
A list of standard and specialised tests is summarised in Table 2. Routine blood cell count and blood smear cytology should be sent to laboratories with experience in equine clinical pathology. A complete haemogram can provide information about systemic conditions such as systemic inflammation and anaemia (the former is common in chronic cases of systemic inflammation). Iron, fibrinogen and serum amyloid A can provide further information about the presence of systemic inflammation (Corradini et al, 2014). Serum biochemistry provides an overview of major organ function and damage if present. Low levels of albumin and total protein is usually a result of losses, rather than a decrease in production. Hypoproteinaemia can be caused by protein-losing enteropathies. Protein loss is associated with several changes including mucosal inflammatory infiltrates, villus atrophy, altered epithelial permeability and lymphangiectasia (Craven and Washabau, 2019). Proteins can also be lost in third spaces like the peritoneum or the thoracic cavity. Another cause of protein loss can be renal failure. Lack of production of albumin is not evident in horses until severe liver dysfunction occurs. In cases of hypoalbuminaemia and hypoproteinaemia, a faecal test should be performed along with serological testing for tapeworms. If cyathostomines are suspected, daily faecal samples for five consecutive days should be obtained. Alternatively, fresh non-refrigerated faecal samples for culture should be submitted for larval search. However, this test might be unreliable if infestation is mild to moderate.
If an underlying condition is identified at this point in the examination, the clinician should try to address it. Further testing may be carried out to confirm or rule out these. Ultrasonographic examination of the abdominal cavity can provide important information in cases of weight loss, such as increases in peritoneal fluid, thickened small or large intestine, intra-abdominal masses or abscesses, or changes in parenchymatous organs such as the liver, kidneys, spleen or suprarenal glands. Thoracic ultrasonography can provide evidence of pleural or pulmonary primary and secondary disease. Endoscopy and gastroscopy can provide evidence of gastric and oesophageal diseases, as well as functional and structural disorders that may affect deglutition. In cases of diarrhoea, faecal culture or polymerase chain reaction testing (for Salmonella spp.) and toxin detection tests for Clostridium difficile and C. perfringens should be performed. Other causes of diarrhoea should also be considered.
Specialised testing
If the aetiological factor remains elusive, further diagnostic tests can be undertaken. A peritoneal fluid sample analysis is a relatively simple test to perform in horses. It can provide important information, including evidence of peritoneal reactivity, inflammation, neoplasia and others. A normal peritoneal fluid analysis does not rule out pathology. Both glucose and D-xylose absorption tests are used to test absorption through the gastrointestinal tract.
Glucose and carbohydrate absorption tests
The glucose ‘tolerance’ test is relatively simple and cost-effective. Horses are given 1 g/kg body weight of glucose as a 20% solution via nasogastric tube after a period of fasting. Total malabsorption is diagnosed if blood glucose levels fail to reach an increase of at least 15% of the basal glucose measurement, and partial malabsorption is suspected when glucose peak is between 15-85% of the basal glucose level.
The xylose absorption test is more reliable. Endocrine testing might be indicated, particularly in geriatric patients, to assess for pituitary pars intermedia dysfunction and hyperthyroidism. The preferred method for testing for pituitary pars intermedia dysfunction is the thyrotropin-releasing hormone stimulation test in late summer and early autumn. This is recommended for horses with clinical signs; testing in subclinical or mild cases is currently not recommended. Further research is needed to determine whether early diagnosis would be beneficial or not (Kirkwood et al, 2022). Hyperthyroidism is a rare condition in the horse. In most cases, thyroid enlargement is caused by adenomas and hyperplasia which do not cause alterations in serum thyroid hormone levels (Breuhaus, 2011). Functional thyrotropin-releasing hormone or stimulation tests are required to investigate thyroid diseases in horses (Breuhaus, 2011).
To further evaluate renal function, additional tests may be required. If azotaemia is detected it is important to measure urine-specific gravity. An animal with azotaemia and isosthenuria (urine-specific gravity: 1008-1016) will likely have renal azotaemia. If urine-specific gravity is >2025 then prerenai azotaemia is likely. The serum:urine creatinine ratio is another way to differentiate renal from prerenai azotaemia. Urine reagent strips are a quick way to obtain information on several parameters related to renal health. However, the strips are either for use in humans or dogs and are poorly sensitive and poorly specific for proteinuria in horses, and thus unreliable for measurement of urinary pH. For the measurement of urine-specific gravity, a refractometer is preferred. Ketonuria is rarely described in horses, and the utility of the rest of the parameters usually available for measurement with urine strips has not been evaluated in horses. However, pygmenturia or haematuria, leucocytes and urine cytology with urine examined within 1 hour of collection is ideal, but is often impractical in ambulatory settings. Refrigeration until delivery to laboratory facilities can be done, but the effects of storage on the urine sample must be considered (for example, cell lysis or cast dissolution). The addition of 40% ethanol or 10% buffered formalin will help prevent cell lysis. However, these additives will not stop cast dissolution over time. Symmetric dymethylarginine is offered at some laboratories, although further research needs to be done in order to critically assess its utility in horses (Gratwick, 2021). However, Galen et al (2022) found that symmetric dymethylarginine results were more sensitive that creatinine, urine specific gravity, urinary gamma-glutamyl transferasercreatinine ration in urine and fractional excretion of sodium in a group of horses with acute kidney injury caused by non-steroidal anti-inflammatory drug toxicity. However, since the test is commercially available and reference ranges have been stablished, this marker can be used judiciously in specific cases (Galen et al, 2022).
In horses with evidence of hepatic disease, liver biopsy is indicated. Abdominal radiology is a sensitive method for the detection of enteroliths and sand enteropathy in horses (Ruohoniemi et al, 2001; Maher et al, 2011).
Duodenal, rectal and intestinal biopsies
If there is evidence of malabsorption or intestinal involvement, duodenal, rectal or a full thickness intestinal biopsy is likely to be the next step. Endoscopic biopsies have the advantage of being a non-invasive technique. The gastroscope can be advanced into the pyloric antrum and the duodenum, and several biopsies can be obtained under sedation. These biopsies can be targeted to the affected areas. The main limitation of this technique is that biopsies are superficial and can only target the most proximal end of the duodenum. This can only sample mucosa and, in the best cases, also the submucosa. Orientation of the biopsy is usually distorted, which limits the ability of pathologists to interpret them (Hostetter, 2022). The success rate for the identification of lesions in cases of chronic intestinal inflammation has been reported to be around 50% (Boshuizen et al, 2018).
Rectal biopsies have the advantage of being relatively easy to obtain under sedation in the standing horse. The percentage of diagnostic rectal biopsies for chronic intestinal inflammatory conditions varies from 30-80% (Lindberg et al, 1996; Boshuizen et al, 2018; Hostetter and Uzal, 2022). Samples can be obtained at wrist level (in the retroperitoneal space) or deeper into the rectum. It is likely that the risks associated with a deeper biopsy are not outweighed by any increase in diagnostic accuracy of deeper rectal biopsies. Intestinal full thickness biopsies have the advantage of providing the possibility to select the section of affected gastrointestinal tract and allow for the evaluation of the full thickness of the intestine. This is usually the last test performed, as it is invasive, carries additional risks and costs, and increases recovery time. Full thickness biopsy can be obtained via laparotomy under general anaesthesia. Alternatively, samples can be obtained via standing laparoscopy. A key factor to consider when interpreting endoscopic or full-thickness biopsies is the overall quality and the number of biopsies (Hostetter et al, 2022). In addition, biopsy samples should be evaluated by an experienced pathologist.
KEY POINTS
- Protein-calorie malnutrition remains the most common cause of weight loss in horses.
- Importance should be given to the diet, feeding management, social interaction, time of the year and physiological status.
- Objective assessment of weight and body condition score changes should be pursued.
- An exhaustive physical examination including oral examination and rectal palpation should be performed in all horses with ongoing weight loss.