

Back pain, either primary or secondary, is a common presenting problem in equine practice and it can be difficult to negotiate these cases successfully. This is the result of a number of issues, including the difficulty of pinpointing the site of back pain, limited treatment options and the expectations of owners who often have preconceived ideas of what is wrong with the horse and their own opinions on treatment modalities. However, a logical approach to the case can provide a good framework for investigation of possible back pain, giving all parties the maximum chance of a successful outcome. The aims of the clinician are to: establish whether back pain exists; what is the cause of the back pain; and how it can be treated. This article provides an overview of these areas.
Does back pain exist?
History
The history of a horse with back pain can be very varied as, like humans, different individuals interpret pain and manifest discomfort in different ways. Some recurring themes in the histories of horses with proven back pathology include a reluctance to be saddled or mounted, irritation when touched or groomed over the back and a reluctance to work forwards under saddle, often kicking out in transitions. In severe cases, the horse may be described as reluctant to lie down or to roll, or as becoming difficult to shoe.
Clinical examination
A clinical examination of the back is required to ascertain whether back pain exists. Horses with back pain will have tension of the longissimus dorsi muscle and will likely show resentment to pressure on the affected area. Hypertrophy of the epaxial muscles in the lumbar region is commonly detected in horses presenting for back pain but, in the author's experience, this finding usually reflects hind limb or pelvic pain rather than primary back pathology. It is important to remember that the horse will naturally dip (ventro-flex) the saddle region when pressure is applied here and that this dipping away does not itself indicate pathology. A good clinical examination tip is to use the (non-ink) end of a pen and to run the pen down the midline of the back with firm pressure to see what the response to the pressure is. A horse with back pathology often does not want to ventro-flex the spine and will resent being asked to do so – horses may become agitated and attempt to move away from the examiner, may throw the head up or buck. In some cases, the horse will drop the back away from the examiner by lowering the pelvis and hind legs rather than ventro-flex the spine.
Dynamic examination
The clinical signs of back pain/pathology during the dynamic examination are varied, non-specific and not pathognomic. Add to this the contribution of the owner/trainer and the whole clinical scenario can become quite difficult. The usual lameness workup work flow is adequate to show clinical signs of back pain (i.e. walking and trotting in a straight line and lunging on soft and hard surfaces). Additionally, it is very useful to see the horse ridden if safe to do so. During the examination, the vet should be observant for signs of back pain and for signs of any lameness.
The clinical signs of a horse with back pain can vary, from subtle loss of performance to severe resistance to being ridden, including rearing and dangerous behaviour. However, in the author's experience, bucking is not as commonly associated with proven back pathology as many other clinical signs, as bucking requires significant back movement and a hallmark of horses with back pain is back rigidity.
Some horses become reluctant to allow saddling or mounting. When ridden, horses may show clinical signs of back stiffness with the back held very rigid, a reluctance to work ‘over the back’ to accept the contact, a reluctance to canter and a ‘bunny-hopping’ gait or becoming disunited in canter. In addition, horses may swish their tail, have a raised head carriage and be generally reluctant to work.
Having taken a good history, examined the horse and observed the horse moving, the vet should be able to decide whether the horse does or does not have back pain and whether any lameness is present.
What is the cause of the back pain?
Once back pain is recognised, the next step in the diagnostic pathway is to identify the cause of the back pain and to ascertain whether it is a result of a primary condition of the back or whether it is secondary to other orthopaedic pathology. Causes of back pain are osseous pathology and/or soft tissue pathology. The more common osseous pathologies include over-riding dorsal spinous processes (ORDSP) or ‘kissing spines’, osteoarthritis of the articular process joints of the spine and ventral spondylosis. Unlike in dogs, disc disease is extremely rare in the horse, although lumbo-sacral disc pathology is recognised. Soft tissue pathologies include damage to the key ligaments of the back, myopathies and muscle strains, and inflammation.
The usual first step in finding the cause of the back pain is to take radiographs of the back. These radiographs are invaluable in showing ORDSP (using latero-lateral (LL) radiographic views), osteoarthritis of the articular process joints (20° oblique views) and ventral spondylosis (LL views). In the author's opinion, it is very important to make sure that a complete set of radiographs is obtained, to include the views of the articular process joints, as pathology here is common, is often associated with ORDSP and will alter the treatment and prognosis for the horse.
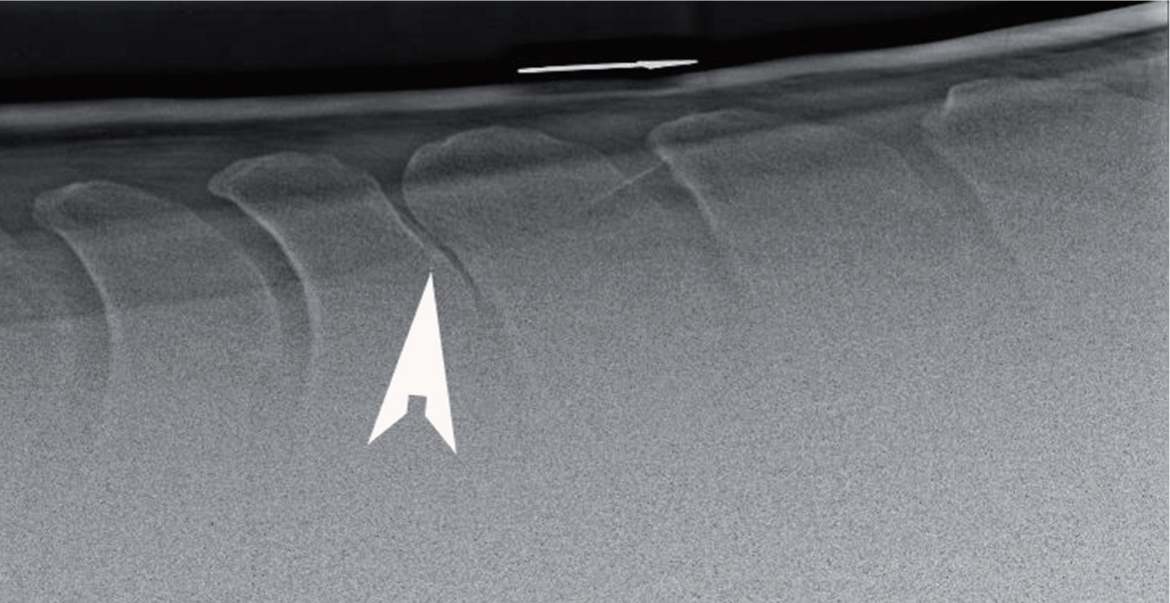
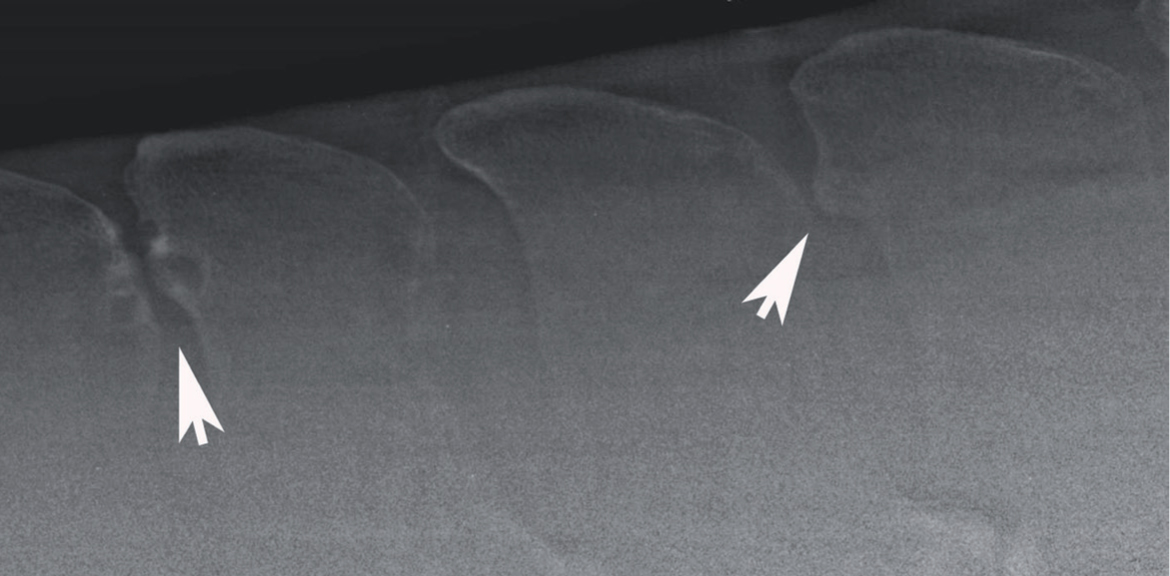
ORDSP are one of the commonest abnormalities detected on radiographs of the back. These ORDSP vary in severity and can be graded either to reflect changes in the back as a whole (grades 1–3) or changes at individual dorsal spinous processes (grades 1–4) (Denoix and Dyson, 2011). In the mildest cases, evidence of impingement can be deduced from sclerosis on adjacent dorsal spinous processes even though on the radiograph there is space between the dorsal spinous processes (Figure 1). It is hypothesised that this sclerosis reflects dynamic contact between adjacent dorsal spinous processes that may occur during back movement. Increasing severity of ORDSP leads to loss of the inter-spinous space, remodelling of the adjacent dorsal spinous processes including osteolysis, changes in shape (Figure 2) and eventually overriding and, in some chronic cases, false joint formation.
The diagnosis of ORDSP using radiography is not straightforward. First, take care not to miss all affected ORDSP – in one study, the most severe lesions of ORDSP were between T11–L1 and L4–5 (Clayton and Stubbs, 2016). While ORDSP in the T11–L1 region are easily diagnosed, it is very difficult to image the lumbar region with some of the X-ray equipment in use in equine practice, but lesions at these sites must be considered as sources of pain, and efforts should be made to image these sites to give a complete picture of the pathology.
Having observed ORDSP on radiographs, be aware that ORDSPs are commonly found in horses with no thoracolumbar pain (Zimmerman et al, 2012). Indeed, one post mortem study showed that 70% of normal horses had 1+ ORDSP (Clayton and Stubbs, 2016). Therefore, further diagnostic imaging such as the use of nuclear scintigraphy should be considered in order to identify areas of active remodelling (Zimmerman et al, 2012). However, the true clinical significance of ORDSP can only be proven by using local diagnostic analgesia, and its use has been associated with a successful treatment outcome (Brown et al, 2020). Local anaesthetic is injected at the site(s) of ORDSP and the response assessed with the horse performing its normal activity. One word of warning here, however – local anaesthetic can diffuse the short distance to articular facet joints and give a false positive result. Therefore, a small volume of local anaesthetic should be used (2–3 ml) to infiltrate this region and the results assessed within 15–20 minutes after injection.
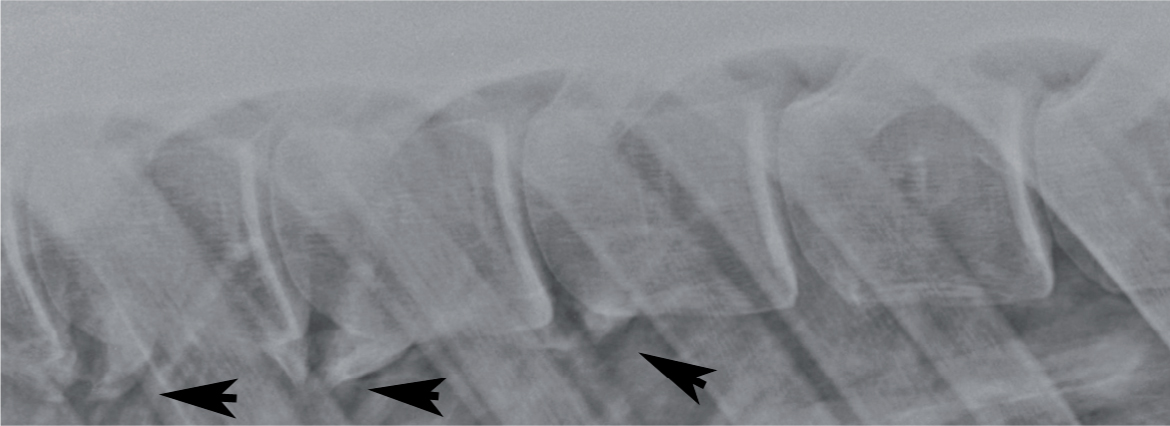
Osteoarthritis of the articular process joints is a fairly common finding in horses with back pain (Girodroux et al, 2009). Oblique radiographs are required to visualise the articular process joints (Figure 3) and confirmed using nuclear scintigraphy and ultrasound. The presence of osteoarthritis is considered to be a significant finding in horses, with osteoarthritis rarely being found in horses with no thoracolumbar pain (Girodroux et al, 2009). Osteoarthritis is often found in conjunction with ORDSP and the presence of both pathologies worsens the prognosis for the horse.

Ventral spondylosis is seen on the LL radiograph at the base of the vertebral bodies (Figure 4) and is an uncommon finding (found in 3–4% of horses with back pain). The clinical significance of ventral spondylosis is unknown, although if such a lesion is shown to be remodelling on nuclear scintigraphy (i.e. it is ‘active’), it may be considered more likely to be painful (Meehan et al, 2009). However, it is not possible to undertake diagnostic local analgesia of the ventral region of the vertebral bodies and so clinical judgement must be used in the interpretation of the presence of ventral spondylosis at the current time.
Soft tissue pathology of the back is often diagnosed but, as with ORDSP, the clinical significance of findings can be difficult to prove. Causes of soft tissue pathology are often ill defined and non-specific, but both desmitis of the supra-spinous ligament and focal myopathy are well recognised. Diagnosis of soft tissue pathology is primarily done by ultrasonography. Ultrasonography of the supraspinous ligament is easily performed in the mid-line of the back and both hypoechogeneic and hyperechongeneic lesions are commonly found. However, as with ORDSP, care must be taken in the interpretation of any pathology as it has been shown that many lesions in this structure can be found in normal horses (Henson et al, 2007), although pathological lesions, associated with heat, pain and swelling, are also seen. As with ORDSP, the use of local analgesic techniques to prove the clinical significance of any lesions found is very important. A less common cause of soft tissue back pain is a focal primary myopathy of key muscle groups that can cause back pain and/or poor exercise intolerance as a result of polysaccharide storage myopathy (Quiroz-Rothe et al, 2002) or myofibrillar myopathy (Valberg et al, 2017). Diagnosis of myopathy is often a diagnosis of exclusion, as focal lesions do not necessarily lead to increases in creatine kinase and aspartate aminotransferase levels, and so a speculative muscle biopsy may be required, which can be hard to convince the client to do. However, it is worth just keeping an open mind about possible myopathy in the absence of any other clinical findings.
How can back pain be treated?
The treatment of back pain in the horse, depends of course, on the diagnosis. Treatment of ORDSP is conservative, medical or surgical. Conservative treatment relies on rehabilitation and schooling to encourage the horse to develop a strong ‘top line’ and core strength. Shockwave therapy to provide analgesia may also be considered. In mild cases this can be successful; however, most cases require at least medical treatment such as the intra-lesional injection of corticosteroid (in conjunction with neurolytic agents such as Sarapin®) at the site of ORDSP. This can provide relief from clinical signs for a variable period of time depending on the individual.
Surgical treatments for ORDSP have been well described (Walmsley et al, 2002; Coomer et al 2012; Jacklin et al, 2014) and are routinely performed, both standing and under general anaesthesia. These treatments range from resection of large portions of the offending dorsal spinous processes to removal of the specific portions that are in contact (subtotal ostectomy). Other methods of treating ORDSP include transection of the intra-spinous ligament (Coomer et al, 2012) to release tension on the dorsal spinous processes, which provides good pain relief and has an excellent cosmetic result. The prognosis for a horse that has undergone surgery for ORDSP is, of course, only as good as the diagnostic work up – if ORDSP is the cause of the clinical signs, then removing the ORDSP will theoretically remove the clinical signs. However, failing to diagnose concurrent pathology such as osteoarthritis of the articular process joints or myopathy will lead to a poor clinical outcome and the surgery will be considered to have failed. An accurate prognosis for the different surgical techniques available for the treatment of ORDSP can be difficult to give; however, reported rates for a return to former athletic function of between 52% and 85% (up to 3-year follow-up) have been published for transection of the intra-spinous ligament (Derham et al, 2019; Prisk and Garcia-LÓpez, 2019) and approximately 80% for subtotal ostectomy (Brink, 2014; Jacklin et al, 2014).
Treatment of osteoarthritis of the articular process joints is difficult. Injections of corticosteroids into the affected area under ultrasound guidance can provide relief from clinical signs and the use of bisphosphonates to successfully treat this condition has been described (Coudry et al, 2007). However, the prognosis for a return to former athletic function is poor. The treatment of ventral spondylosis is extremely difficult, as there is limited access to the ventral aspect of the spine for direct injection. In cases in which it is considered that an active spondylosis is causing pain, giving the horse sufficient time to allow the spondylosis to form and mature may improve the clinical signs once the bone formation has stabilised.
The treatment of soft tissue injuries depends on the cause. Local injections of anti-inflammatory medication can reduce the impact of supra-spinous ligament desmitis and nutritional changes may help horses with myopathy, depending on the specific histological changes detected at biopsy. More generalised muscle strains will be helped by rest and physiotherapy.
Conclusions
A logical approach to assessment and an appreciation of the most common causes of back pain and how to recognise them allows the clinician to approach back cases with confidence.
KEY POINTS
- Diagnosing back pathology requires a detailed history, clinical examination and the use of thorough diagnostic techniques.
- Over-riding dorsal spinous processes are not necessarily a cause of back pain.
- The presence or absence of osteoarthritis of the articular process joints should be established before proceeding to medical treatment and/or surgery.
- Treatment of back pain requires a multi-modal approach.